The Sydney classification for injuries following polypectomy is a system used to categorize and describe the severity and type of complications that can occur after the removal of polyps from the gastrointestinal tract, particularly the colon. The system provides a standardized way to document and communicate the extent of these injuries, which can help guide management and treatment decisions.
The Sydney classification includes the following categories:
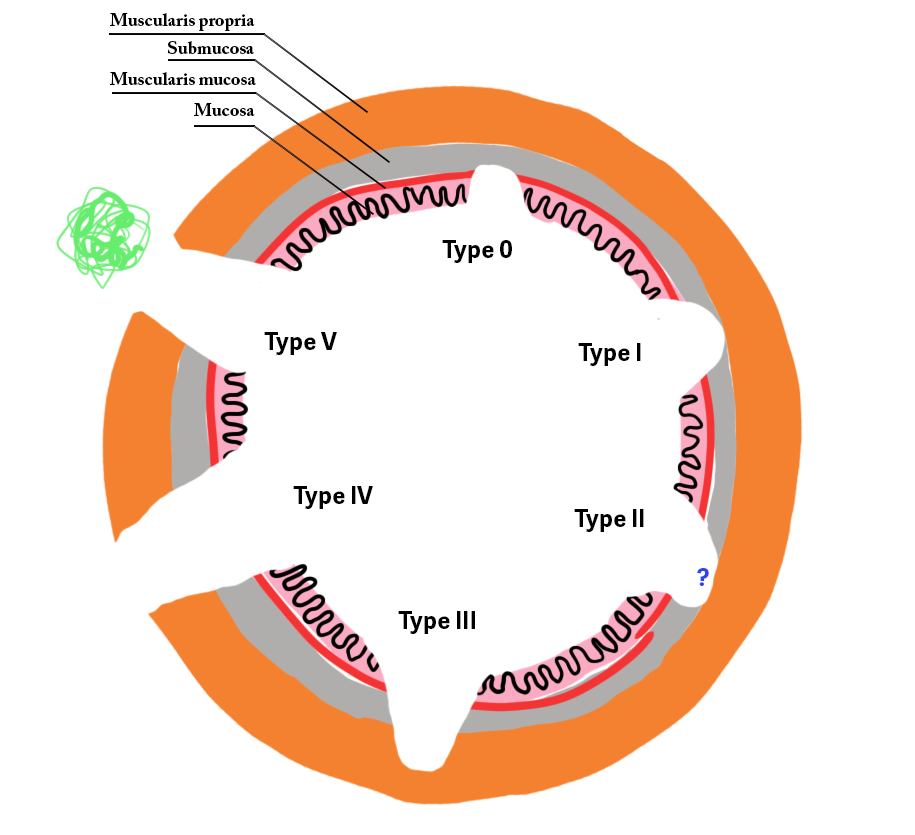
- Type I: Minor injury (mucosa and submucosa)
- Type II: Injury into the muscularis propria without perforation
- Type III: Full-thickness injury with microperforation
- Type IV: Full-thickness perforation with a visible defect
- Type V: Severe injury with extraluminal leakage of luminal contents
The Sydney Classification for deep mural injury (DMI) following endoscopic mucosal resection (EMR) categorizes the extent of injury to the gastrointestinal wall, particularly the colon, into different types based on depth and severity. Here are the types in the Sydney Classification:
Type I Deep Mural Injury:
- Description: Minor injury limited to the mucosa and submucosa.
- Characteristics: This type involves superficial damage that does not extend into the muscularis propria. There is no perforation, and the integrity of the muscle layer is maintained.
- Clinical Implications: Generally considered low risk for complications, healing is typically straightforward with conservative management.
Type II Deep Mural Injury:
- Description: Injury extending into the muscularis propria without perforation.
- Characteristics: This type involves a deeper injury that reaches the muscle layer but does not cause a full-thickness perforation. The muscularis propria shows visible damage but remains intact.
- Clinical Implications: May require closer monitoring and management to prevent further complications such as delayed perforation or bleeding.
Type III Deep Mural Injury:
- Description: Full-thickness injury with a microperforation.
- Characteristics: This type involves a full-thickness injury to the bowel wall with a small, localized perforation that might not be immediately obvious but can be detected on close inspection or imaging.
- Clinical Implications: Requires careful management, often with hospitalization and possibly antibiotics or surgical intervention if the perforation leads to significant clinical symptoms.
Type IV Deep Mural Injury:
- Description: Full-thickness perforation with a visible defect.
- Characteristics: This type represents the most severe form of injury, with a full-thickness tear that creates a visible defect in the bowel wall. This can lead to the escape of luminal contents into the peritoneal cavity.
- Clinical Implications: This is a medical emergency requiring immediate intervention, usually surgical repair, and comprehensive supportive care to manage peritonitis or sepsis.
Type V Deep Mural Injury:
- Description: Severe injury with extraluminal leakage of luminal contents.
- Characteristics: Involves severe damage that results in significant leakage of bowel contents outside the lumen, often associated with extensive tissue injury and potentially widespread peritoneal contamination.
- Clinical Implications: This represents a critical condition necessitating urgent surgical intervention, extensive decontamination, and aggressive supportive measures to manage systemic infection and stabilize the patient.
References:
- The Sydney classification for deep mural injury (DMI) following endoscopic mucosal resection (EMR) includes various extents of DMI, with type III being muscularis propria injury (target sign) and type IV/V being perforation without or with contamination.1
- The classification system was used in a study involving 911 lesions in 802 patients, where DMI signs were identified in 83 patients (10.3%), with type III-V DMI occurring in 3.0% of patients.
- The study found that type III-V DMI was associated with identifiable risk factors such as transverse colon location, en bloc resection, and high-grade dysplasia or submucosal invasive cancer
Related articles:
*Hiroshima classification
*Haggitt level
*Kikuchi
*KUDO pit pattern
*Paris
*SANO classification
*SMSA classification for prediction of complexity for endoscopic resection